










Services on Demand
Journal

Article
 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO
Related links
-
 Similars in
SciELO
Similars in
SciELO
Share

 Permalink
PermalinkMemorias del Instituto de Investigaciones en Ciencias de la Salud
On-line version ISSN 1812-9528
Mem. Inst. Investig. Cienc. Salud vol.21 no.1 Asunción 2023 Epub Nov 21, 2023
https://doi.org/10.18004/mem.iics/1812-9528/2023.e21132302
Case Report
Localized tooth surface loss: Dahl technique with direct free-hand resin composite build-ups in the anterior sector. Case Report

1Universidad Católica “Nuestra Señora de la Asunción” Facultad de Ciencias de la Salud, Carrera de Odontología. Campus Itapúa, Encarnación, Paraguay
2Universidad de Cardiff y Vale, Junta de Salud, Gales, Reino Unido
3Universidad de Manchester, NHS Fundación, División de Odontología, Manchester, Inglaterra, Reino Unido
4Real colegio de Médicos y Cirujanos de Glasgow, Escocia, Reino Unido
5Fundación Rotherham, Inglaterra, Reino Unido
6Universidad Tehran De Ciencias Médicas, Tehran, Irán
Tooth Surface Loss (TSL) is defined as a condition in which the wear of the tooth structure is excessive according to age. This pathological loss is commonly related to a combination of factors such as erosion, abrasion, attrition, or parafunction. The Dahl technique is a valid alternative that solves the problems that arise in this type of situation, such as dentoalveolar compensation. This case describes a 63-year-old patient who attended the Dental Hospital of the University of Manchester, referred by his private dentist. At the time of the clinical examination, moderate to severe loss of the palatal and incisal tooth surface located in the anterior sector of the teeth, deep overbite and dental alveolar compensation were found. Direct free-hand restorations were performed from canine to canine. After incisal filling, a posterior open bite of approximately 1 to 1.5 mm was observed. Posterior occlusal contact was completely restored in 3 months.
Keywords: DAHL technique; Loss of tooth surface; Direct Composite; Dento-Alveolar Compensation
La pérdida de superficie dental se define como una condición en la que el desgaste de la estructura dental es excesivo según la edad. Esta pérdida patológica se relaciona comúnmente con una combinación de factores como erosión, abrasión, atricción o parafunción. La técnica de Dahl es una alternativa válida que resuelve los inconvenientes surgidos en este tipo de situaciones como ser la compensación dentoalveolar. Este caso corresponde a un paciente de 63 años que acudió al Hospital Dental de la Universidad de Manchester, derivado por su odontólogo particular. Al momento del examen clínico se constató pérdida moderada a severa de la superficie dental palatina e incisal localizada en el sector anterior de los dientes, sobremordida profunda y compensación alveolar dental. Fueron realizadas restauraciones directas a mano alzada de canino a canino. Luego del relleno incisal se constató una mordida abierta posterior de aproximadamente 1 a 1,5 mm. El contacto oclusal posterior fue restablecido totalmente en 3 meses.
Palabras clave: Técnica de DAHL; Pérdida de superficie dental; Restauraciones directas; Compensación Dento-Alveolar
A perda da superfície dentária é definida como uma condição em que o desgaste da estrutura dentária é excessivo de acordo com a idade, essa perda patológica está comumente relacionada a uma combinação de fatores, sendo eles: erosão, abrasão, atrito ou parafunção. Uma abordagem restauradora nestas situações representa um desafio para a reabilitação oral principalmente pela Compensação dentoalveolar. A técnica de Dahl é uma alternativa válida para resolver este problema. Este caso corresponde a um paciente de 63 anos que procurou o Hospital Odontológico da Universidade de Manchester, encaminhado por seu dentista particular. No momento do exame clínico, observou-se perda moderada da superfície dentária no setor anterior, sobremordida profunda e compensação alveolar dentária. Foram realizadas restaurações diretas da mão livre do canino para o canino. Após o enchimento incisal, observou-se mordida aberta posterior de aproximadamente 1 a 1,5 mm. O contato oclusal total foi restabelecido em 3 meses.
Palavras-chave: Técnica DAHL; Perda da superfície dentária; Restaurações diretas; Compensação dentoalveolar
INTRODUCTION
Tooth wear (tooth surface loss or TSL) is defined as a condition in which tooth structure loss is excessive according to age. Physiological wear is related to the loss of 0.02-0.04 mm of enamel per year, when this rate is exceeded and creates discomfort and aesthetic concerns, pathological wear is implicit1. Pathological loss is commonly related to a combination of factors, these being: erosion (non-bacterial chemical processes) abrasion (wearing away not related to mastication) attrition (the mechanical wear of chewing or parafunction, produced by the contact of the surfaces of the teeth). In addition, it is associated with changes in tooth morphology, hypersensitivity, and deficiency of function. However, asymptomatic cases are also common2.
The management of mandibular anterior teeth such as incisor and canine represent a challenge for oral rehabilitation. As this loss of substance is slow and allows dentoalveolar compensation, the contact between antagonistic arches is maintained, leaving no interocclusal space for restorations. An alternative to solve this problem is the placement of composite restoration at a high vertical dimension, known as the Dahl technique3.
Dahl's concept was introduced in 1975 as a method to manage localized tooth loss4. This concept follows two types of axial movements of the teeth, comprising 40% of anterior teeth intrusion and 60% of posterior teeth extrusion5. In the posterior sector, the reestablishment of occlusal contact is expected in months; according to Dahl 4-6 months. However, Poyser et al. reported longer period than 18-24 months4,5.
When using Dahl's approach, case selection is of paramount importance. Especially consideration such be placed to avoid engaging restoration in a supra-occlusal position in patients with periodontal problems or bone loss (6).
In the report of the current clinical case, a patient with localized dental surface loss due to pathological wear was presented, treated by Dahl approach, with direct freehand composite restorations in the anterior sector, following several steps which will be explained in detail below.
CASE PRESENTATION
A 63-year-old male patient presents at the Oral Rehabilitation Clinic of the University of Dentistry in Manchester, England (Central Manchester University Hospitals NHS Foundation Trust). As the only underlying pathology reported is high blood pressure, which is controlled with Losartan 100mg x 1 taken daily. The patient was referred by his dentist due to his moderate loss and wear of non-decayed tooth tissue. His class 2 division 2 occlusion was also a cause for concern. The patient has received previous treatment that includes anterior composite restoration, which have failed, and reports feeling unhappy with the bite that he describes as "tight bite". The upper anterior implant was placed 17 years ago, in addition, he was given a 'plate' (dentures of a single tooth) to try to correct a bite that tested her for 4 weeks, but then discontinued its use.

Figure 1. Intraoral Preoperative Photographs. A. Deep overbite, front view. B. Moderate to severe loss in the ant eriorinferior sector. C. and D. Side views of the initial situation. E. and F. Occlusal views of wear in the upper (E.) and lower (F.) arches.
At the time of the clinical oral examination, moderate tooth surface loss, located palatine in the anterosuperior teeth, and moderate to severe loss in the anteroinferior sector were observed, mainly due to wear and tear, secondary to erosion. Mostly dentate maxilla, implant retained crown in the upper right central, partially dentate mandible (missing first molars of both hemiarches). Traumatic incisive relationship Class II Div. 2. Deep overbite, not traumatic for soft tissues, but with noticeable tooth wear. Palatine surfaces of the upper incisors that are occluded against the lower incisors. Space between the premolars on both sides (lower arch). Right and left group function during lateral excursions. Dental alveolar compensation. Periodontal status within normal ranges.
Extraoral examination revealed no masses or scars; neck and mandibular muscles within normal limits, no lymph node abnormalities were detected and the Temporo Mandibular Joint (TMJ) without clicks or any joint sound present, ranges of motion were within normal.
To prepare the treatment plan, casts were studied and consultations with other colleagues were carried out to evaluate the benefits of orthodontic treatment and the possible incisal lengthening. Since the patient had lesions of considerable extensions, the proposal of the Dahl technique would allow us the necessary incisal lengthening through direct restorations, thus keeping the intervention as minimal as possible with minimal or no dental preparation at all where indicated (7). This would be favorable because it would improve the aesthetics and function of the patient. If the patient was not happy or if there was an early failure of the restoration, then indirect restorations would be performed in a second phase.
Treatment was started, following the different phases of the rehabilitation protocol, an emergency phase was not necessary. During the stabilization phase, oral hygiene instructions were given, with the recommendation of the correct use of interdental brushes, fluoride toothpaste and soft toothbrush. Continuing with the restorative phase, primary impressions were taken with stock trays and alginate as impression material in upper and lower arches, facial arch registration for articulator mounting, bite registration in CR (Centric Relation). In the following session, a minimal invasive procedure was applied, the exposed dentin was removed to improve adhesion, cleaning all surfaces with pumice, water, and a cup. Direct freehand composite restorations were carried out in the anterior sector from canine to canine in the lower and upper arch. No wax-up was used. Isolation of the operative field was performed using rubber-dam, cotton rolls and suction devices. When needed, matrix and wedges were used. A three step etch-and-rinse adhesive system was applied according manufacturer´s instruction: 37% phosphoric acid (Gluma, kuzler) universal adhesive (gluma univeersal bond, kuzler). A nanohybrid composite material (Venus, Kulzer) was applied to restore the anatomical lost form of the treated teeth. A led polymerization unit was used to light cure the composite. Occlusal contacts were positioned in the center of the restoration accordingly to long axis of the teeth.
After the incisal filling, a posterior open bite of approximately 1 to 1.5 mm was observed and measured with a ruler on mounted casts and intra oraly. The post-treatment vertical dimension of occlusion was estimated by the amount of composite required to restore the anatomical proportions of the worn dentition.
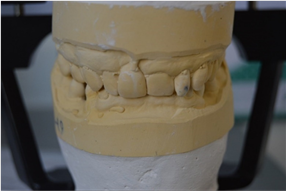

Figure 3. Immediate postoperative. A. Incisal restorations. B. Palatine restorations. C. and D. Posterior dis-occlusion in right and left side views.
The first control had to be performed in the following week of the restorations, however, the patient was on family vacation, therefore, the patient was seen after one month of the restoration application, by this date part of the subsequent occlusion was already partially restored. Posterior dental contacts were evaluated using Shim Stock occlusal sheet and occlusal strip. After a month, subsequent contacts were re-established, but the Shim stock was still not trapped between the two arches (6).

In the splint fitting appointment *3 months after Dahl technique, occlusal control with strips showed a total reestablishment of posterior occlusal contact. .

Annual reviews were encouraged during the Maintenance Phase.
The use of Dahl's concept made it possible to provide natural anterior teeth without major loss of structure. Aesthetics and function were also improved with direct restorations. Posterior occlusal contacts were established in approximately 3 months and the patient received a soft occlusal splint. The patient was extremely satisfied with the result.
The patient was instructed with oral hygiene measures, frequency, technique, and timing of toothbrushing. The patient was also informed about the need for maintenance of the restorations. The patient was advised to wear the soft splint when sleeping and monitor daytime bruxism.
DISCUSSION
Some advantages when using direct restoration within the Dahl technique, allow you to choose this treatment option over other more invasive ones, which include the prevention of a greater loss of dental substance in an already compromised dentition, the simplicity of placement, aesthetic, economical and predictable result when humidity control is maintained. Also, failures are susceptible to simple maintenance in the form of repairment or replacement of the restoration and is a suitable technique in the young patient. Although these restorations may not last more than 3 to 5 years, maintenance is relatively simple. In addition, restoration can be used as a diagnostic tool. The acceptable level of tolerance for pulp tissues and minimal abrasion to antagonistic surfaces made this technique the best indicated6,8,9.
We must also tell the patient the disadvantages with respect to the selection of the material, in his case, related to the contraction of polymerization, which can culminate in marginal leakage and staining. In the same way, an accelerated wear rate is expected (compared to metals/ceramics), especially in the area where your restoration will meet into contact with cast metal porcelain crowns. There is also the possibility of fracture(s). Discoloration is likely to occur; even though the patient does not smoke8.
In a 10-year study by Smales et al., the survival rate of direct restoration using the Dahl technique on anterior teeth was reported at 5.8 years; Survival in a case like that presented (of mandibular anterior teeth) was 94% at 2.5 years and 85% at 7 years10.
In this case, a direct freehand restoration of teeth with composite resin was carried out and according to Poyser it is the most adaptable and maintainable technique. Alternative direct techniques with the use of a vacuum-formed matrix from a diagnostic wax-up have been suggested to facilitate the direct placement of multiple composite fillings9.
In this clinical case, Dahl's concept made possible the rehabilitation of the anterior sector without compromising the dental structure. Likewise, aesthetics and lost function were restored with direct non-invasive restorations. Posterior occlusal function was restored in approximately 3 months and total patient satisfaction was achieved with the result obtained. Unfortunately, due to issues related to the pandemic and the suspension of clinical care, it was not possible to continue with a follow-up of this case.
REFERENCES
1. Rashid H, Hanif A, Nasim M. Tooth surface loss revisited: Classification, etiology, and management. Journal of Restorative Dentistry [Internet]. 2015 [cited 2023 Apr 29]; 3(2): 37. Doi: 10.4103/2321-4619.156643. https://www.researchgate.net/publication/276440927_Tooth_surface_loss_revisited_Classification_etiology_and_management [ Links ]
2. Warreth A, Abuhijleh E, Almaghribi MA, Mahwal G, Ashawish A. Tooth surface loss: A review of literature. Saudi Dent J [Internet]. 2020 Feb 1 [cited 2023 Apr 29]; 32(2): 53-60. Doi: 10.1016/j.sdentj.2019.09.004 [ Links ]
3. Al-Khayatt AS, Ray-Chaudhuri A, Poyser NJ, Briggs PFA, Porter RWJ, Kelleher MGD, Eliyas S. Direct composite restorations for the worn mandibular anterior dentition: a 7-year follow-up of a prospective randomised controlled split-mouth clinical trial. J Oral Rehabil 2013 [cited 2023 Apr 30]; 40 (5): 389-401. https://onlinelibrary.wiley.com/doi/10.1111/joor.12042 [ Links ]
4. DAHL BjL, Krogstad O, Karlsen K. An alternative treatment in cases with advanced localized attrition. J Oral Rehabil [Internet]. 1975 Jul 1 [cited 2023 Apr 29]; 2(3): 209-14. https://onlinelibrary.wiley.com/doi/full/10.1111/j.1365-2842.1975.tb00914.x [ Links ]
5. Poyser NJ, Porter RWJ, Briggs PFA, Chana HS, Kelleher MGD, Poyser N. The Dahl Concept: past, present and future. Br Dent J 2005; 198(11): 669-76; cuestionario 720. Doi: 10.1038/sj.bdj.4812371 [ Links ]
6. Hemmings KW, Darbar UR, Vaughan S. Tooth wear treated with direct composite restorations at an increased vertical dimension: results at 30 months. J Prosthet Dent [Internet]. 2000 Mar 1 [cited 2023 Apr 29]; 83(3): 287-93. Doi: 10.1016/s0022-3913(00)70130-2. http://www.thejpd.org/article/S0022391300701302/fulltext [ Links ]
7. Satterthwaite JD. Tooth surface loss: tools and tips for management. 1012968/denu201239286 [Internet]. 2017 Jun 20 [cited 2023 Apr 29]; 39(2): 86-96. https://www.magonlinelibrary.com/doi/10.12968/denu.2012.39.2.86 [ Links ]
8. Banerji S, Mehta SB, Opdam N, Loomans B. Practical procedures in the management of tooth wear. [cited 2023 Apr 29]; [cited 2023 Apr 29]; https://www.wiley.com/en-us/Practical+Procedures+in+the+Management+of+Tooth+Wear-p-9781119389965 [ Links ]
9. Poyser NJ, Briggs PFA, Chana HS, Kelleher MGD, Porter RWJ, Patel MM. The evaluation of direct composite restorations for the worn mandibular anterior dentition - clinical performance and patient satisfaction. J Oral Rehabil [Internet]. 2007 May 1 [cited 2023 Apr 29]; 34(5): 361-76. https://onlinelibrary.wiley.com/doi/full/10.1111/j.1365-2842.2006.01702.x [ Links ]
10. Milosevic A, Burnside G. The survival of direct composite restorations in the management of severe tooth wear including attrition and erosion: A prospective 8-year study. J Dent.2016 Jan 1; 44: 13-9. Doi: 10.1016/j.jdent.2015.10.015 [ Links ]
Responsible Editor: María Eugenia Galeano Dinatale . Universidad Nacional de Asunción, Instituto de Investigaciones en Ciencias de la Salud, San Lorenzo Paraguay. Email: ccdiazabc@gmail.com
Author contributions
Author 1: Data/information collection, Data analysis/discussion, Literature review and Manuscript preparation.
Received: May 04, 2023; Accepted: November 01, 2023
 Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
