










Serviços Personalizados
Journal

Artigo
 texto em
texto em  Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO
Links relacionados
-
 Similares em
SciELO
Similares em
SciELO
Compartilhar

 Permalink
PermalinkCirugía paraguaya
versão On-line ISSN 2307-0420
Cir. parag. vol.46 no.3 Asunción dez. 2022
https://doi.org/10.18004/sopaci.2022.diciembre.28
Case report
Recurrence of gallbladder adenocarcinoma in laparoscopic trocar port. A case report

1Ministerio de Salud Pública y Bienestar Social. Hospital Nacional. Departamento de Cirugía. Itauguá, Paraguay.
2Centro Educativo Superior en Salud. Departamento de Extensión e Investigación. Ypacarai, Paraguay
El cáncer de vesícula es un hallazgo incidental en el 0,5% a 2,3% de todas las colecistectomías por litiasis vesicular. Se debe sospechar en toda tumoración sobre las cicatrices de puertos de trocares. El seguimiento histopatológico postoperatorio es importante para el diagnóstico. Se presenta el cuadro clínico de un paciente sometido a colecistectomía laparoscópica previa (18 meses), con tumoración umbilical recidivante por cáncer de vesícula.
Palabras clave: Neoplasias de la Vesícula Biliar; Metástasis; Laparoscopía; Recurrencia
Gallbladder cancer is an incidental finding in 0.5% to 2.3% of all cholecystectomies performed due to vesicular lithiasis. It should be suspected on any tumors present on the scars of trocar port sites. Postoperative histopathological follow-up is important regarding its diagnosis. This is the case report of a patient treated with previous laparoscopic cholecystectomy with recurrent umbilical tumor due to gallbladder cancer.
Keywords: Gallbladder. Neoplasms. Metastasis. Laparoscopy. Recurrence,
INTRODUCTION
The rate of gallbladder cancer is between 0.5% and 2.3 % of all cholecystectomies performed due to vesicular lythiasis.1,2,3Preoperative diagnosis is difficult to achieve because no specific symptoms can be found. Therefore, diagnosis is achieved through anatomo pathological examination.1,2One of the rarest complications in laparoscopic cholecystectomy is metastatic seeding of peritoneal implants in laparoscopic ports.4 This clinical entity is exclusive of laparoscopic surgery.1,2,3The way of presentation is the appearance of a tumor on painless previous scars, without obstructive symptoms. Differential diagnosis is needed in the presence of abdominal wall hernias and primary neoplastic diseases.5 The most widely accepted mechanisms of tumor spread through trocar port sites are gallbladder perforations, tumor cell spreads due to the action pneumoperitoneum, the chimney phenomenon, and extraction without gallbladder bag.3,6
CASE REPORT PRESENTATION
This is the case of a 59-year-old man who presented with pain around the umbilical region of 3-day evolution. Patient had not been radiated. Pain partially recedes with common analgesics. The patient complains of constipation (though not of gases) of 3-day evolution, no nausea or vomiting. The physical examination reveals the presence of an umbilical tumor of 15 cm of maximum diameter with erythematous skin and inflammatory changes, irreducible, incoercible, painful to superficial palpation, with mate sound, without variation with the Valsalva maneuver, and scarce hydro-aerial noises on the tumor (see Figure 1).

The patient’s past medical history is having been the carrier of such painless tumor (“hernia”) for the past 6 months with rapid and progressive growth.
Also, he says that the underwent a laparoscopic cholecystectomy 18 months ago at a different center without postoperative follow-up.
Additional diagnostic examinations were conducted: the abdominal x-ray performed in the standing position revelaed no signs of bowel occlusion. The soft tissue ultrasound performed revealed the presence of an umbilical hernia with content blockage of left para-lateral location suggestive of left colon with significant parietal and hypoechogenic swelling. Vascular pattern was seen when the color Doppler ultrasound was used (see Figure 2).
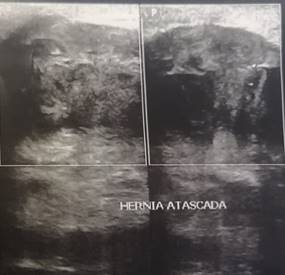
Figure 2. Soft tissue ultrasound showing a left para-lateral umbilical hernia with content blockage.
The exploratory laparotomy performed revealed the presence of a solid petrous tumor in the periumbilical region of 15 cm x 12 cm x 10 cm in size whose spread was limited in depth to the skin, and the subcutaneous cellular tissue. The aponeurosis of the anterior sheath of rectus, anterior rectus muscle, and parietal peritoneum without invasion of the cavity or any loop adherences was confirmed as well. Large tumor resection was performed with en bloc resection of rectum muscles. Abdomen remained opened using the Bogotá bag technique with abdominal wall deficit of nearly 15 cm x12 cm (see Figure 3). Afterwards, treatment with VAC-type negative pressure system was used.

Pathology report confirmed the presence of an abdominal wall tumor with compromise of fibroadipose and musculoskeletal tissue due to moderate-to-poorly differentiated infiltrating adenocarcinoma (grade 2-3) of 15 cm of maximum diameter with extensive areas of necrosis, lymphovascular emboli, and perineural invasion. Finding was compatible with tumor of vesicular origin from previous surgery (see Figure 4)
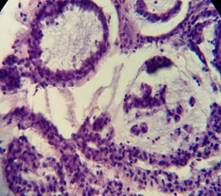
Figure 4. Anatomopathological features of the tumor. Atypical cellular nuclei with scarce cytoplasm making up the glandular lumen (Courtesy of Dr. Rocio Rizzi, Anatomical Pathology Unit, Itauguá National Hospital).
The anatomic pathology correlation with previous cholecystectomy was established. The patient had not the pathology report after failing to attend his postoperative monitorization follow-up that already reported on the presence of a 5.5 cm infiltrating adenocarcinoma of vesicular body. Extensive poorly differentiated areas with infiltration of all layers of vesicular walls up to the perimuscular fibroconnective tissue were described. These were located, at least, 1 mm away from the hepatic bed. No serous invasion was observed whether vascular or perineural. Stage pT2b.
DISCUSSION
Metastasis of gallbladder cancer to umbilical trocar port sites is rare1,2,3, and diagnosis should be achieved through anatomopathological examination2. In the presence of suspected preoperative gallbladder cancer, the use of videolaparoscopy approach is contraindicated.1,2,3On the other hand, differential diagnosis is important with other tumors of the abdominal wall5.
This case was highly suggestive of para-umbilical hernia with content blockage, not tumor relapse. Histopathological follow-up of cholecystectomy and early procedures reduce the appearance of peritoneal seeding4 that was not performed on this patient since he never went to any postoperative follow-ups.
Implants in trocar port sites take between 2 weeks and 4 years before they make their appearance since the early procedure. Their appearance means advanced disease.4,6 Treatment is surgical with wide tumor resection that improves the patient’s quality of life but does not change prognosis or survival.1,2,6
REFERENCES
1. Cano C. Adenocarcinoma de pared abdominal y carcinoma insospechado de vesicula biliar: un tributo de la cirugía laparoscópica. Revista hispanoamericana de Hernia, 3, 100-104. [ Links ]
2. Gorron M, Cadermil N, Del Valle C, Diaz J. metástasis en puerto umbilival por adenocarcinoma incidental de vesícula Biliar. Cua-dernos de Cirugia, 2018; 18(1), 38-42. [ Links ]
3. Vergnaud J, Lopera C, Penagos S, Palacios D, Vazquez J. Metastasis en el puerto laparoscópico posterior a colecistectomía laparos-cópica. Rev Colomb Cir, 2000; 15(2), 52-55. [ Links ]
4. Machado I, Cruz J, Lavernia J, Carbonell F. Lesiones ocu-pantes de espacio en pared abdominal (no herniaria). La visión del pató-logo. Revista Hisponoamericana de Hernia, 2015. 3(3), 85-94. [ Links ]
5. Martin E, et al. Diagnostico Tardio de Carcinoma oculto de Vesicula biliar por implante metastásico en puerto laparoscópico. Cirugia Espalñola, 2016.582-584. 5. Singla S, Budhijara S. Port site metastasis after laparoscopic cholecystectomy. The Indian Journal of Surgery, 2009; 71(1), 41-42. [ Links ]
6. Singla S, Budhijara S. Port site metastasis after laparoscopic cholecystectomy. The Indian Journal of Surgery, 2009; 71(1), 41-42. [ Links ]
4Authors’ contributions: MAAW: study idea, data collection and mining, case report preparation, study design, critical review of the manuscript and final approval of case report. GIPG: study design, data assessment, case report review and final approval. CPB: study idea, data and clinical health record curation, manuscript critical review and final approval.
Received: June 07, 2022; Accepted: September 18, 2022
 Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
