











 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Similars in
SciELO
Similars in
SciELO 
 Permalink
Permalink
Introduction
Diabetes mellitus is a group of metabolic disorders characterized by chronic hyperglycemia1. T2DM, constituting 90%2) of cases, is associated with risk factors such as advanced age, obesity and physical inactivity3. In addition, a higher prevalence is observed in women with a history of gestational diabetes, hypertension, and/or dyslipidemia as well as in certain ethnic groups. The disease tends to develop progressively after the age of 40 and usually has a strong genetic basis. Lack of obvious symptoms often leads to delayed diagnosis, which can result in chronic complications4,5.
Before T2DM, many people had already developed prediabetes, with high glucose levels, but not high enough for diagnosis. There are often no clear symptoms that can result in late diagnosis and long-term complications. Although not specifically treated, reducing glucose levels and other risk factors may be beneficial6. Research has shown that weight loss and moderate exercise can reduce the risk of developing T2DM by 58%. Effective prevention is achieved by intervening in the lifestyles of high-risk individuals7,8, highlighting the importance of early detection9.
The Finnish Diabetes Risk Scale, known as FINDRISK, is the first widely used predictive risk scale for T2DM. This scale consists of eight simple questions with a pre-established score that estimates the probability of developing T2DM over the next 10 years10. The scale has been adapted and validated in several populations in Europe, America, and Asia11-17.
According to a recent study carried out in Encarnación, Paraguay, with a sample of 460 adult patients, 71.74% were at risk of developing DM2 when using the FINDRISK test (18). Furthermore, data from the most recent National Risk Factor Survey carried out by the Ministry of Public Health and Social Welfare19 showed a higher prevalence of diabetes in women, with 12.6% compared to 7.6%. recorded in men. It stands out that 10.6% of the total population of Paraguay suffer from this disease. Regional statistics also reveal that one in ten women develop diabetes during pregnancy, with poor diet, overweight, and obesity being factors that contribute to the appearance of this disease during this stage20.
Considering the previous considerations, the main objective of this work is to predict the risk of contracting diabetes in female physicians, nurses, and administrative staff of a reference hospital in the city of Asunción. The FINDRISK test helps us determine the probability of developing DM2, known risk factors, and, in this way, try to prevent or delay its onset through education and lifestyle changes that serve to care for the disease. their own health, as well as those of their family members and patients.
Methods
This descriptive cross-sectional observational study was conducted from June to August 2022 in a maternal and child referral hospital in Asunción, Paraguay. Physicians, nurses, and administrative staff who voluntarily signed an informed consent form were invited to participate in the questionnaire. Women with a known diagnosis of diabetes mellitus and pregnant women were excluded from the study because glucose metabolism presents important differences at this stage.
The selection and recruitment of participants were carried out in a non-probabilistic manner for convenience; however, a reference sample size estimation was carried out. Considering that the Asunción Hospital has a total of 759 working women and taking into account a previous study16, 7.8% of the participants showed a "high risk" of developing diabetes according to the FINDRISK test, it was determined that a minimum of 99 participants were needed with a confidence level of 95% and a margin of error of 5%. To account for possible data loss, the sample size of 109 participants was estimated. As the focus of the study was to visualize the risk of gestational diabetes in women, it was decided to focus exclusively on the female population.
Data were collected using the FINDRISK test to assess the diabetes risk. The collection was carried out using an electronic form hosted on a specific website created for this purpose. The form included an informed consent form followed by a questionnaire consisting of eight questions addressing variables such as age, sex, body mass index (BMI), waist circumference, level of physical activity, consumption of fruits and vegetables, history of high blood pressure (HBP) or use of medications for it, altered fasting glucose levels, first-degree family history (parents and siblings) with a diagnosis of DM2, in addition to two additional questions about work occupation and the availability of health insurance.
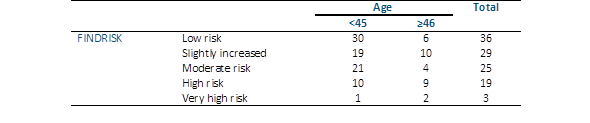
According to the responses, the scoring scale is as follows (10, 14): < to 7: Low Risk (RB), 7-11: Slightly Elevated Risk (RL), 12-14: Moderate Risk (RM), 15-20: High Risk (RA), >20: Very high-risk (RMA).
According to ADA21, if the score obtained is high (> 14), medical control is recommended. Statistical analyses were performed using Epi Info version 7. Descriptive statistics were used to calculate the frequencies and means. In addition, statistical tests were performed, including the Mann-Whitney U test, to analyze the relationship between the variables age (dichotomized) and risk level of DM2. The dichotomization of the age variable was carried out considering the reproductive age threshold defined by the World Health Organization (WHO), dividing the participants into two groups: those under 45 years of age and those aged 46 years or older22. The Kruskal-Wallis test was used to evaluate the relationship between occupation variables and the risk level of DM2.
The protocol for this research was approved by the FOUNA Ethics Committee (Report No. 40/22) and authorized by the hospital’s Medical Directorate. The ethical principles of autonomy were observed, with voluntary participation and informed consent, beneficence, non-maleficence (no harm was caused, and the results were accessible to the participants, promoting preventive behaviors), and respect for the privacy of the study subjects (confidentiality of data was always maintained).
Results
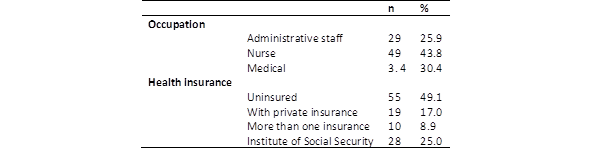
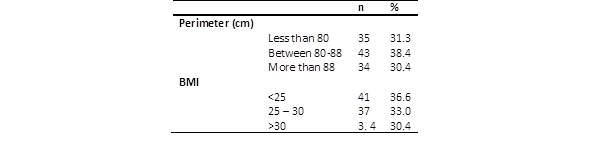
A total of 113 women responded to the questionnaire (response rate of 15%), of which 1 was excluded because of incomplete data. Finally, the total number of participants was 112, of which 43.8% were nurses, and more than 49% did not have health insurance. The age of the participants varied between 23 and 65 years, with an average age of 39.9 ± 9.5 years (Table 1). The waist circumference of 80-88 cm. This was the most frequent (38.4%). Of the participants, 33% were overweight (Table 2).
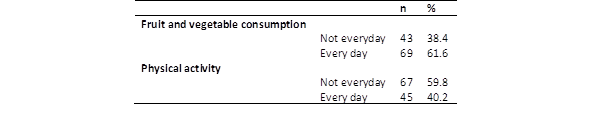
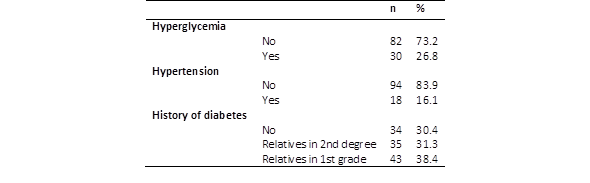
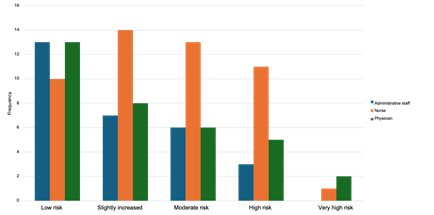
More than 50% of the surveyed respondents consumed fruits and vegetables daily. However, almost 60% of the patients did not perform physical activity every day (Table 3). While most reports had no history of hyperglycemia and hypertension, more than 38% of first-degree relatives had a history of diabetes (Table 4). Overall, it is possible to observe that 67.9% of those surveyed have some risk of developing DM2 in the next 10 years (Table 5). According to the total number of women surveyed, 22 of the FINDRISK test, a high or very high risk of developing DM2 in the coming years. Respondents aged ≥ 46 years had a significantly higher risk (Mann Whitney; p=0.08) (Table 6). Regarding occupation (physician, nurse, and administrative staff), no significant differences were found in the risk of developing diabetes (p=0.06). However, three administrative staff members presented a high risk of developing DM2, and none of them showed a very high risk (Figure 1).

Discussion
Several recent studies have shown that DM2 can be prevented by intervening in the lifestyle of people at high risk of suffering from it7,9,23. Even in individuals with prediabetes, early treatment can return blood glucose levels to the normal range (remission)9. Early identification of patients at high risk for DM2 is crucial for implementing effective preventive actions9,24.
Of the total number of women surveyed in this study, almost 20% had a high or very high risk of developing DM2 in the coming years according to the FINDRISK test. This finding is consistent with similar reports in Brazil17) and Spain25. In a study conducted in Cuba and published by Naranjo et al.13, it was observed that the very high risk was notably higher, reaching 10.5%. One of the main discrepancies with the present study is the habit of consuming healthy food. While more than half of the Paraguayan women reported consuming fruits and vegetables daily, only 13% of the participants in the Cuban study did so. When evaluating the results of the present study, it is important to keep in mind that the sample consisted only of women, unlike the aforementioned research reports that included both sexes. This sex difference could make comparisons difficult, as previous research has indicated that healthy eating habits can vary significantly between men and women26.
The worldwide obesity rate has almost tripled since 197527. In this study, more than half of the respondents were overweight or obese. Genetic and environmental factors are directly associated with adipose-tissue dysfunction. Adipocyte hypertrophy, hypoxia, and inflammation may act as important mediators in the pathogenesis of obesity-related complications. Ectopic fat accumulation, particularly visceral obesity, is postulated to result from adipose tissue dysfunction, suggesting a direct connection between altered cellular composition and insulin sensitivity28. Currently, metabolic syndrome is considered the direct result of abdominal fat determined by waist circumference9,23,29. Considering the WHO parameters30, in this study, more than half of the participants had a waist circumference that corresponded to a high and very high risk of developing DM2. Very similar results were reported in studies from the neighboring country Brazil12,17 and Colombia16. These data show that obesity is not only a problem at the country level but also affects a large part of the region. According to reports, in 2016, the estimated prevalence of overweight and obesity at the regional level was 62.5% (64% in men and 61% in women), the highest among all WHO regions31.
Weight reduction through a dietary plan in accordance with current recommendations in terms of fat quality; fiber intake; increased use of whole grain products, fruits, and vegetables; and increasing physical activity can prevent T2DM7. In the present study, it was observed that although 61.6% reported eating fruits and vegetables daily, 59.8% did not engage in physical activity. The variables of physical activity and the consumption of fruits and vegetables did not increase the predictive power of DM2 in the same way as age, waist circumference, history of blood glucose, and family history. However, with a healthy lifestyle, even people with genetic susceptibility to diabetes can avoid the symptomatic phase of the disease10.
A person is more likely to develop T2DM if they have hypertension or a history of hyperglycemia32. Less than 20% of participants reported taking medications for hypertension. However, according to data from the Ministry of Public Health and Social Welfare, the prevalence of hypertensive patients is currently approximately 38.6%19; therefore, we should not rule out under-registration in the population studied. We must remember that hypertension is known as the “silent killer” since it rarely causes symptoms33.
The observation of an increased probability of DM2 in the age group ≥46 years suggests that despite the presence of other factors, age continues to be one of the determining factors in the risk analysis according to the FINDRISK test. Therefore, emphasizing the adoption of a healthy lifestyle in the younger population is crucial to establishing healthy habits for the future, while in the older population, it is important to warn about the greater predisposition to develop the disease. Despite not finding significant differences, it was observed that female employees, including hospital secretaries and cleaners, presented a lower frequency of risk in all categories. Importantly, work activities that involve repetitive physical movements such as cleaning can contribute to a higher level of physical activity during work.
The results obtained recently in a similar study carried out in Paraguayan territory18 largely agree with the results obtained in the present study. In both cases, more than 50% of the population had some risk of developing DM2, and more than 60% had an increased BMI. Similar values were also found regarding the history of hypertension, whereas the figures for the history of glycemia in the present study were higher. It is important to note that the aforementioned study was carried out in a population of men and women, whereas this study focused only on the female population. These comparisons underscore the consistency of findings across different populations and highlight the importance of considering differences in sample composition when interpreting the results.
However, some methodological limitations must be mentioned. Although the FINDRISK test was used to assess diabetes risk, this tool is based on self-reports and may be subject to perception bias on the part of participants. Furthermore, other possible risk factors, such as a family history of other chronic diseases or socioeconomic status, were not evaluated. However, when using statistical tests to analyze associations between variables, it is important to keep in mind that this analysis can only identify association relationships and not causality.
Diabetes in Paraguay currently represents 10.6% of the total population19. Currently, nearly 200 million women are living with diabetes worldwide, and this number is predicted to increase to 313 million by 204034. The present work seeks to make visible the high predisposition to DM2 found even in female workers at a reference hospital, who, it could be presumed, are in some way more exposed to information on the prevention and care of general well-being. Through the study, the participants were able to learn about the risk of T2DM and remember that adopting healthy habits, such as a balanced diet and regular exercise, can help prevent it.
Preventing diabetes through lifestyle modification not only has individual benefits but can also generate positive impacts on healthcare systems and society by reducing the burden of chronic diseases and improving health and quality of life.

