











 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Similars in
SciELO
Similars in
SciELO 
 Permalink
Permalink
Introduction
Infectious intestinal diseases (diarrhea) are a major cause of morbidity and mortality worldwide. In 2015, it constituted the ninth leading cause of death for all ages; in 2017, in children under five years old, it was the third leading cause of death and has been shown to be the cause of at least 8 million deaths in low- and middle-income countries, with a cost of economic losses of at least $6 trillion1-3. In children under 5 years of age, the number of diarrhea episodes per year varies from 3,3 to 9 episodes4. In addition to mortality, acute or chronic diarrhea affects the development and growth of children, mainly during the first two years of life, correlating with poor school performance and low wages in adulthood5.
Most diarrheas have infectious etiology, being the main pathogenic agents; viruses (Norovirus, Rotavirus, Astrovirus and enteric Adenovirus) bacteria (Salmonella spp., Shigella spp., Campylobacter spp., Vibrio spp., E. coli diarrhea spp., Aeromonas spp., Yersinia spp., among others) and, less frequently, parasites (Cryptosporidium spp., Giardia spp., Cyclospora spp., Microsporidium spp., Entamoeba hystolitica, Balantidium coli)5. According to the World Health Organization (WHO), in low-income countries, the most common pathogens in low-income countries are Rotavirus, Escherichia coli, Cryptosporidium spp., and Shigella spp.4.
In general, diarrhea is self-limiting, and although deaths from diarrhea have declined sharply in the past two decades, it is estimated that by 2050, 1.4 million people will die from diarrheal diseases6, mainly due to the great social and health inequities in low-income countries. Thus, in these countries, the social determinants of health form a complex multifactorial network in which risk factors related to the individual, environment, and animals are intertwined7. 80% of the risk factors for diarrhea are related to poor environmental conditions such as basic sanitation, hygiene habits, poor quality and low coverage of drinking water, and in children, malnutrition, and dehydration4,8,9.
Furthermore, in addition to poor environmental conditions, there is a lack of access to and poor quality of health systems. In developed countries, deaths due to diarrhea are infrequent, unlike in underdeveloped countries, where hospital admissions are observed due to complications such as severe dehydration and renal failure, especially in elderly patients. This population may present with diarrhea in up to 20% of cases during the treatment of diabetes mellitus6. Therefore, in recent years, the use of oral rehydration salts has been emphasized to prevent dehydration, which is the main cause of mortality in children and the elderly4. Paraguay ranks the lowest in the Human Development Index (HDI), with a value of 0.728, ranking 103 out of 189 countries and territories. Its ranking is lower than the average of countries with a high HDI and the average of Latin America and the Caribbean10. Therefore, it presents great social and health inequities, which have repercussions on the prevalence of certain infectious diseases such as diarrhea.
Acute childhood diarrhea constitutes in Paraguay, the fourth cause of mortality in children under 5 years old and according to the General Directorate of Health Surveillance (GDHS) of the Ministry of Public Health and Social Welfare (MSPBS), notifications for diarrhea were increasing from 49,750 cases for the year 2015 to 226,413 for the year 2018. Broadly speaking, except for the year 2015, in the other years, most of the cases were in those older than 5 years11-15. In other studies, it was observed that 40.1% of the cases corresponded to diarrhea in children under 5 years of age, and 59.8% of the cases were observed in children over 5 years of age16,17. The objective of this study was to describe mortality due to diarrhea in Paraguay between 2015 and 2019.
Methods
The study was descriptive, ecological, cross-sectional, and temporally retrospective. The geographical scope was composed of 17 Paraguayan Departments, including Asunción, the capital city. The study period was from 2015 to 2019. Sampling was nonprobabilistic for consecutive cases. The considered variables were sex, marital status, educational level, age, and 17 Paraguayan Departments. The place of residence of the deceased was considered as the origin of the cases. Deaths from non-nationals were excluded from the calculation of the rates.
Deaths due to diarrhea of infectious etiology were considered, which were classified in the ICD-10 as infectious intestinal diseases, including cholera (A01), typhoid and paratyphoid fevers (A02), shigellosis (A03), other bacterial intestinal infections (A04), other bacterial food poisoning not elsewhere classified (A05), amebiasis (A06), other intestinal diseases due to protozoa (A07), intestinal infections due to viruses and other specified organisms (A08), diarrhea, and gastroenteritis of suspected infectious origin (A09)18. The data source used was the open-access data available on the website of the General Directorate of Strategic Health Information (GDSHI) of the Ministry of Public Health and Social Welfare (MSPyBS)19.
Crude and adjusted rates (100,000 per capita) were calculated. Excel and EPI INFO 7.0 were used. For statistical analysis of nominal and categorical variables, frequencies were calculated and expressed as percentages. Averages were calculated for the numerical variables. Gross and adjusted rates were also calculated using population data from the National Institute of Statistics (NIS) and the World Health Organization's standardized population standard20-22. Regarding ethical criteria, as this was a research study with a secondary data source that did not involve human subjects, the protocol of the present study did not require the approval of the Research Ethics Committee.
Results
From 2015 to 2019, 495 people died of diarrhea of infectious etiology, the main etiology being diarrhea and gastroenteritis of presumed infectious origin (A09), which constituted 95.56% of the deaths. During this period, there were no deaths due to diarrhea caused by cholera (A01), typhoid and paratyphoid fevers (A02), shigellosis (A03), amebiasis (A06), or viruses (A08) (Table 1).

Table 1 Etiology of deaths due to infectious intestinal diseases (diarrhea) according to the cie - 10, paraguay (2015-2019) (n=495).
The year with the highest number of deaths was 2019, with an adjusted rate of 1.83 per 100,000 people and 23.84% of cases, and the year with the lowest prevalence was 2015, with an adjusted rate of 1.36 per 100,000 people (Table 2). As for the monthly distribution of cases, January and July (9.9%) and October (9.3%) had the highest number of cases (Figure 1). Regarding the age and sex of the deceased, the highest number of deaths occurred in both the earlier and later stages of life. Thus, in children under 5 years of age, most deaths occurred in males. However, in older adults, from 65 years of age onwards, most deaths occurred in the female sex (Figure 2)

Table 2 Annual distribution of infectious intestinal disease (diarrhea) cases, paraguay (2015-2019) (n=495).
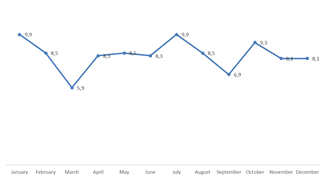
Figure 1 Monthly percentage distribution of infectious intestinal diseases (diarrhea) cases per year, paraguay (2015-2019) (n=495).
The highest number of deaths occurred in both the earlier and later stages of life. Thus, in children under 5 years of age, most deaths occurred in males. However, in older adults, from 65 years of age onwards, most deaths occurred in the female sex (Figure 2). Regarding the demographic characteristics, 51.72% were women. In terms of age, the average was 50.8 years. When analyzing the distribution according to age categories, 30.91% of the cases occurred in those over 80 years of age and 28.28% were under 5 years of age (Table 3).
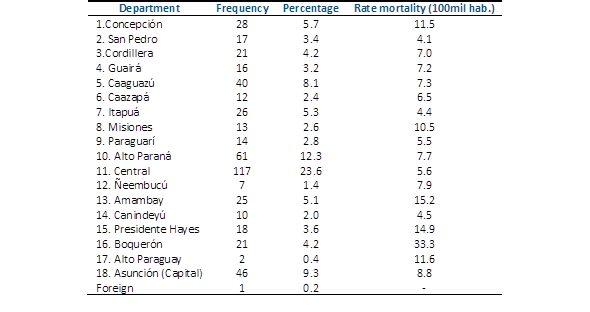
Regarding the area of residence of the deceased, the highest mortality rates occurred in the Departments of Boquerón (33.3 per 100 000 inhabitants) and Amambay (15.2) (Table 4).
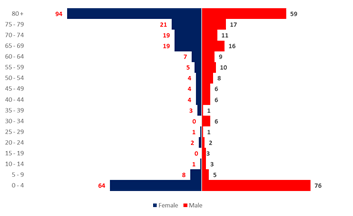
Figure 2 Distribution of deaths from infectious intestinal diseases (diarrhea) by age and sex, paraguay (2015-2019) (n=495).
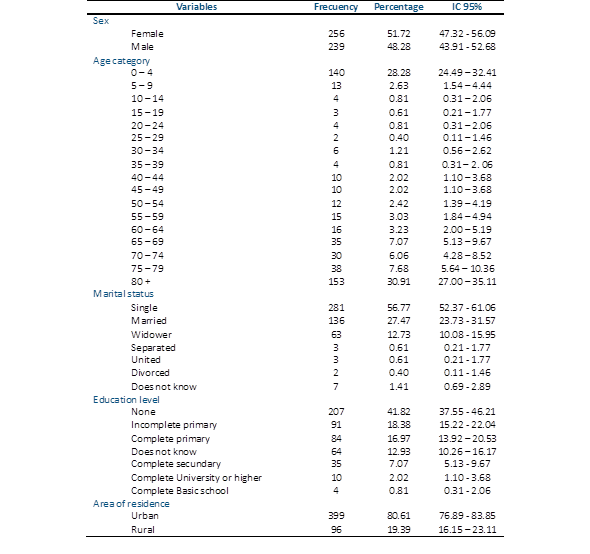
Table 3 Demographic characteristics of patients who died from infectious intestinal diseases (diarrhea), paraguay (2015-2019) (n=495).
Discussion
Infectious diarrhea continues to be one of the main causes of death from diarrhea in Paraguay, and despite efforts, there has been a sustained increase over the years. This could be because notification systems and the quality of death certificates have been improving over time, so that under-registration has been decreasing and the quality of death certificates has improved. Another hypothesis is that this increase is because diarrhea is on the rise due to the persistence of poor conditions related to the environment (hygiene, coverage, and quality of drinking water and sanitary sewage) and to the individual (low or low level of education).
According to data from the Health Services Company of Paraguay (HSCP), drinking water coverage in Paraguay accounts for 80% of the population in urban areas and 33% in rural areas. Drinking water is distributed through a network of pipes that are in very poor condition, causing significant water losses (47% of losses) and leakage inside the network. The HCSP estimates that 300,000 m of pipes must be replaced. The poor quality of these pipes also favors contamination of the water being transported. Another point related to the environment is that there is practically no sanitary sewage system; therefore, there is no wastewater treatment. Asunción, the country's capital, and the metropolitan area have 33% of its population connected to the sanitary sewer system22-25.
As for factors related to the individual, diarrhea has moved from the pediatric population to the geriatric population, since it can be observed that the highest prevalence of mortality occurred at both the early and later stages of life, those over 80 years of age, and those under 5 years of age. This is because this population is increasing among those over 80 years of age. According to INE data, this population currently includes 746,445 people aged 60 and over, of whom 48.3% are men and 51.7% are women26. Even so, it is striking that mortality is due to this pathology since diarrhea, in general, can be cured with good oral rehydration. Further research should be conducted to determine whether this mortality is related to a lack of access to health services.
In this demographic group, acute diarrhea could be due to the prolonged use of broad-spectrum antibiotics or fragility of the immune system27. Most deaths occurred in women aged > 65 years. This could be because they often live alone, have a low educational level, have little or no work activity, face specific age-related problems, and do not attend medical consultations. It could be because it is women who have a longer life expectancy, as well, with a projected 80.7 years for this sex by 2030 according to the WHO27,28.
In children under 1 and 5 years of age, Paraguay presented values that placed it above countries such as Haiti (10%), Nicaragua (8%), Guatemala (7%), and Bolivia (6%), with 14.2 and 16.8 deaths per 1,000 live births, respectively, being one of the main causes of death along with pneumonia and influenza29.
Regarding pathogenic agents, the absence of mortality due to Salmonella spp. and Shigella spp. is striking, as these agents are the most prevalent in diarrhea of infectious etiology. Evidently, these pathogens are agents of morbidity, but not mortality30. In Asunción and the metropolitan area, diarrheagenic Escherichia coli, Rotavirus, Campylobacter spp., Shigella spp., and Salmonella spp. have been described as the most prevalent etiological agents in children under 5 years of age31.
The absence of mortality due to cholera is expected, since Paraguay reported only two cases of this pathogen even during the cholera epidemic. Consequently, Paraguay is considered cholera-free32. However, approximately 1.3 4 million cases of cholera and 21,000-143,000 deaths due to cholera have been reported annually worldwide33.
Regarding mortality due to food poisoning, this could be considered underreported because of the precarious conditions in which many establishments work in this area and the lack of control by the authorities in charge. Epidemiological surveillance in the last two or three decades has shown an increase in the prevalence of foodborne diseases (FBD), with outbreaks of diseases such as salmonellosis, Enterohemorrhagic Escherichia coli infections (EHEC), and hepatitis A. There is little literature on this topic; the only information available reports that between 2015 and 2016, a total of 14 outbreaks of FBD were recorded, with a total of 231 cases, with no deaths reported because of this health event34,35.
There were numbers concerning the monthly distribution of cases; the months with the highest number of cases were January, July, and October. Bacterial diarrhea is more prevalent in the warm summer months, and since no mortality due to viruses was observed in this five-year period, we assumed that the mortality due to diarrhea in July was also due to bacterial agents. Another point to consider is that Paraguay has high temperatures throughout the year. The month of January coincides with work carried out in Argentina, where there were two peaks during the year. One of the peaks occurred during the warm months, with a predominance of bacterial infections, and the other peak occurred during the cold months, where the prevalence of viral diseases was observed36.
Regarding the area of residence, the highest mortality rates (33.3 and 15.2) were in the Departments of Boquerón and Amambay, respectively, both geographically distant from the most complex healthcare centers for better care. In most developed and developing countries, mortality due to diarrhea is no longer a major public health concern. However, in Paraguay, mortality due to diarrhea of infectious etiology continues to be a complex problem that requires an approach based on social determinants of health for its prevention and elimination.

